

By Natsuko Matsukawa
National Flags of DRC and Belgium. (Image Source: Alamy; https://tinyurl.com/mr36jtyz)
1. Introduction
Human African Trypanosomiasis (HAT), also known as African sleeping sickness, is a vector-borne parasitic disease primarily transmitted by the tsetse fly. It is caused by two subspecies of Trypanosoma brucei, which is a protozoan, a single-celled parasitic flagellate: T. b. rhodesiense and T. b. gambiense, with the latter accounting for most human infections[i]. HAT poses a persistent public health challenge across sub-Saharan Africa, where tsetse flies are found and if left untreated, the disease is fatal. The Democratic Republic of the Congo (DRC) has historically accounted for the majority of global HAT cases, representing 61% of cases in the last five years. As shown in Figures 1 and 2, below, the number of new HAT cases in DRC far exceeds that of other countries. Over the past century, four major epidemics have occurred, including the 1998 epidemic, which reported nearly 40,000 cases, with an estimated 300,000 undetected. Thanks to global collaborative efforts, HAT cases have steadily declined worldwide over the past two decades, with only 625 cases of T. b. gambiense in the world reported in 2018. While the DRC still reports the highest number of new cases globally, the figures have dropped significantly – from a peak of 26,318 in 1998 to just 394 in 2023[ii]. HAT was included in WHO’s 2012 roadmap for Neglected Tropical Diseases(NTDs), which aimed to completely interrupt transmission in Africa by 2030, with 2020 set as the goal for global elimination of gambiense HAT as a public health problem (defined as fewer than one new case per 10,000 people in at least 90% of foci) [iii]. In 2018, the WHO confirmed that those reduction targets had been met[iv]. However, despite recent medical advancements and international aid, the goal of elimination by 2030 remains a major challenge.
This paper analyzes the historical trajectory of aid interventions for HAT in the DRC, examining how colonial policies, international cooperation, and social and structural factors have shaped both the disease’s spread and the responses to it. By assessing the broader impacts of past interventions, this analysis aims to inform more effective decision-making in future policies and programs.
The study explains how colonization is related to HAT epidemics in DRC and divides the interventions into two periods: aid interventions in early-mid 20th century and current interventions. During the colonial era, Belgian rule had both direct and indirect effects on the spread of HAT, with strict and sometimes coercive methods achieving partial success. After independence, political instability led to a resurgence of the disease. However, subsequent international cooperation and medical advancements greatly reduced the spread of HAT. These efforts exemplified the potential for global public health coordination while also exposing deep-rooted barriers and challenges in current aid interventions.
The significance of this analysis extends beyond the specific case of HAT, offering insights into the interplay of historical, social, and structural factors in disease control. This approach highlights the necessity of framing health challenges not simply as medical issues, but as complex social problems rooted in various determinants. This historical analysis contributes to ongoing discussions on preventing the resurgence of HAT in the DRC and other regions, while also informing the design of more inclusive and sustainable public health interventions for neglected tropical diseases in similarly vulnerable areas.
2. Colonialism: 1885-1960
The struggle with HAT in the DRC is deeply entwined with its history as a Belgian colony prior to 1960. Even long before the colonial era, HAT was endemic in many parts of Africa, spawning occasional epidemics. African communities had developed a balance between human, domestic, and wild ecosystems possessing knowledge of the habitats of tsetse flies and how to avoid them. However, European colonization disrupted this equilibrium, leading to ecological crises, including famines and epidemics of diseases such as HAT[v]. Beginning in 1885, instead of Belgium itself being the owner of the colony like other European countries, the Kingdom of Kongo, currently the DRC, was ruled as a private possession by King Leopold Ⅱ of Belgium, under the name the Independent Congo State or Congo Free State[vi][vii]. The country endured exploitative, forced labor for ivory, rubber, and palm, mass killings, and gruesome tortures[viii], resulting in approximately 50% of the population dying during this period[ix]. Additionally, displacement, famine, and harsh working conditions as a result of colonization created an ideal environment for diseases like HAT to spread[x][xi].
Due to Leopold Ⅱ’s exploitative and violent rule, strong public opposition in Belgium and investigation by European commission forced him to relinquish control 1908. It became the Belgian Congo as a colony of Belgium. Even after the DRC’s sovereignty was transferred to Belgium, the main target of exploitation shifted to mineral resources[xii], but the structure of exploitation remained unchanged, creating one of the core causes of conflicts, which would be explained later. During this time, the development of non-industrial growth of the Belgian Congo was behind even in Sub-Saharan Africa[xiii]. For example, although several hospitals and infrastructure were constructed in urban areas[xiv], medical policy was quite discriminatory. Access to healthcare for rural and indigenous populations was extremely limited[xv], and this vulnerability facilitated the spread of the disease[xvi].
Even after the DRC’s independence in 1960[xvii], the legacy of the colonial era had a lasting effect on the country. Not only were medical facilities concentrated in urban areas, but the collapse of the healthcare system was exacerbated in the aftermath of independence, due to political and economic instability, which heavily affected the delivery of health services[xviii]. Prime Minister Patrice Lumumba and President Joseph Kasa-Vubu faced military rebellion and separatist movements within weeks of independence. By the summer of 1960, two provinces declared secession, sparking five years of conflict that left over 100,000 dead. In 1965, Mobutu Sese Seko seized power, renaming the country Zaire and ruling through a corrupt kleptocracy, embezzling billions until his fall in 1997. Political instability, especially from the corruption and economic collapse of the Mobutu regime, led to the concentration of the profits from mineral resources among the elite, further hindering the development of healthcare and public infrastructure[xix]. Zaire’s name was changed back to the Democratic Republic of the Congo after the Mobutu regime, and the country suffered through the Second Congo War from 1998 to 2003, which claimed around 3 million lives[xx]. To this day, weak governance generates violent conflicts in the DRC, with an overlap between conflict areas and HAT endemic areas. Not only did conflicts disrupt the control, treatment, and follow-up of HAT, but these also raised the risk of spreading the disease, especially in border areas due to people fleeing from conflicts[xxi]. Due to these conflicts and after a long period of low endemicity of HAT, the control of the disease was no longer a priority, leading to the termination of HAT control programs and the decline of population screening[xxii]. Colonization, corrupt governance, and conflict outbreaks during the colonial period and early independence have severely weakened the DRC’s capacity to provide basic healthcare services. As a result, vulnerable populations have been left unprotected against HAT, allowing the disease to spread widely in both rural and urban areas[xxiii].
3. Aid Interventions in early – mid 20th century
In the first half of the 20th century, efforts to combat HAT in the DRC were primarily led by Belgium, with a focus on treatment and prevention. When the HAT epidemic broke out in Africa, it drew significant scientific and political attention from European colonial powers due to its potential impact on their colonial ambitions[xxiv][xxv]. One of the primary motivations behind European interventions in addressing HAT was, first and foremost, economic concern, as the epidemic worsened labor shortages, significantly impacting transport and colonial exploitation. The early 20th century, being the height of microbiology, also sparked scientific curiosity, driving microbiologists to research HAT. Additionally, the Belgians justified their HAT interventions in the DRC by presenting them as humanitarian efforts to improve public health driven by condescension and racism while these actions also served to legitimize their continued colonial control and economic interests[xxvi]. These motivating factors lead to different priorities and methods in HAT interventions in the DRC compared to interventions in other colonies and in the post-colonial era[xxvii].
In the Congo Free State, due to the difference in how HAT spread, the Belgians adopted a unique approach, prioritizing the treatment of infected individuals to eliminate trypanosomes from their bodies rather than separating humans from tsetse flies, as was done in other colonies. One reason for the difference in treatment was that the spread of HAT accelerated along river routes due to increased population movements as Belgian influence expanded[xxviii]. The Belgian Congo, unlike Uganda and Tanzania, is characterized by sparsely populated rainforests and wetlands, which presented significant challenges for alternative strategies, such as clearing bush and draining swamps. These ecological and demographic factors made such methods unfeasible[xxix]. Following recommendations from a mission from the Liverpool School of Tropical Medicine that King Leopold requested in 1903, the government imposed coercive and oppressive enforcement measures. The sick and those suspected of harboring trypanosomes were confined to isolated camps with poor conditions, where they were given inadequate food and atoxyl injections, while a quarantine zone and movement controls were enforced[xxx][xxxi]. Patients were permanently separated from their families and guarded by soldiers to prevent escape. The oppressive nature of these measures, combined with the forced labor of locals in infected areas and the withdrawal of European doctors during World War I, further exacerbated the epidemic[xxxii].
After a few years, the Belgian authorities shifted to decentralized ambulatory care, deploying mobile medical teams, opening rural clinics, and establishing injection centers – an approach that remains a cornerstone of HAT control efforts in the DRC today[xxxiii][xxxiv]. This initiative, supported by public health services, a dedicated HAT service, and Christian missions, helped bring the disease under control by the 1940s. Additionally, the decline in HAT infections was also aided by the cessation of forced relocations and the easing of social and economic disruptions[xxxv]. Belgium’s interventions were successful in reducing HAT cases and, in this regard, were hailed by other colonial powers as the most effective among European colonies at the time[xxxvi].
Belgian efforts reflected the nature of early to mid-20th-century colonial aid, marked by large-scale, government-driven interventions. While these interventions contributed to the control of HAT in the DRC, they ultimately failed to establish sustainable prevention, leaving the country vulnerable to future outbreaks and resulting in a resurgence of HAT that persisted into the 1990s. Heavy reliance on external funding and medical technology and the coercive nature of measures, such as forced isolation in camps and labor in infected areas, placed colonial interests above the dignity and autonomy of the local population. These problems, despite the numerical success of the intervention, highlight the limitations of colonial-era interventions.
4. Recent Global Aid Interventions
During a resurgence of HAT, 1998 marked the peak of HAT cases in the DRC, with 26,318 new cases reported[xxxvii], as shown in Figure 4 below. This resurgence was largely driven by conflicts and the political, economic, and social instability following independence, which severely hindered disease control interventions and healthcare services[xxxviii][xxxix]. Another factor that led to a resurgence is that HAT became a lower priority, as declining case numbers led to the suspension of many control programs and the neglect of ongoing surveillance[xl][xli], as shown in Figure 5[xlii]. Additionally, although the screening test for HAT, the Card Agglutination Test for Trypanosomiasis(CATT), was developed in the 1970s, its large-scale production proved challenging, and pharmaceutical companies considered discontinuing the production of anti-trypanosome drugs due to low demand[xliii][xliv]. This re-emergence of HAT highlights the intricate interplay of historical, social, economic, and medical factors, compounded by the disease’s inherent susceptibility to resurgence.
Unlike earlier epidemics addressed individually by colonial powers, the late 20th-century HAT epidemic was brought under control through international and public-private coordination. This included the efforts of the WHO, national programs, bilateral cooperation, and NGOs[xlv]. By 1983, global efforts to eliminate HAT in endemic countries had already been initiated by organizations such as the Regional Committee for Africa, the WHO, the United Nations Food and Agriculture Organization, the United Nations Development Programme, the World Bank, and the Organization for African Unity, as stated at the 36th World Health Assembly[xlvi]. However, it was during the peak of the new epidemic in the late 1990s that drew heightened attention from endemic countries and bilateral and multilateral agencies[xlvii]. The WHO responded with a large-scale resolution in 1997 to raise awareness, increase political will, and improve surveillance and access to treatment. Subsequently, in 2000 the WHO launched a global coordination initiative, forming alliances with UN agencies under the PAAT (Program Against African Trypanosomiasis), national governments, and the Organization of African Unity[xlviii].
Through its advocacy campaign, the WHO encouraged the private sector to recognize its responsibilities and subsequently fostered public-private partnerships with pharmaceutical companies, beginning with a pivotal partnership with Sanofi in 2001. Under this agreement, Sanofi has been providing HAT drugs free of charge in endemic areas and contributed over $85 million to the effort. Additionally, the WHO coordinated with NGOs and research organizations such as Doctors Without Borders and the Drugs for Neglected Diseases Initiative (DNDi)[xlix]. The DRC is one of six out of 36 total endemic countries that received support from both the WHO and NGOs, as well as through bilateral cooperation between 2000 and 2009. This support was composed of technical assistance, access to diagnosis, training, and treatment[l]. The development of new medicines also played a key role in reversing the epidemic. Innovations like Nifurtimox-Eflornithine Combination Therapy (NECT), Eflornithine, and Fexinidazole were added to the WHO List of Essential Medicines in 2005 and 2009. This significantly advanced treatment options, simplifying processes[li], as well as collaboration among companies working on HAT drug development[lii].
As a result of these global collaborative efforts, HAT cases have steadily declined worldwide over the past two decades, reaching a historic low. Although the DRC continues to report the highest number of new cases globally, the figures have decreased dramatically from 26,318 in 1998, which was the peak, to only 394 in 2023, as shown in Figure 3[liii]. In the WHO’s 2012 roadmap for neglected tropical diseases (NTDs), complete transmission interruption in Africa was targeted by 2030, with 2020 set as the goal for global elimination of gambiense HAT as a public health problem (defined as fewer than one new case per 10,000 population in at least 90% of foci)[liv][lv]. Consequently, in 2018, the WHO confirmed that reduction targets had been met, placing the ultimate goal of eliminating HAT within reach[lvi]. The success of the large-scale global interventions to combat the resurgence of HAT by international institutions, NGOs, drug companies in the last 20 years demonstrates the effectiveness and importance of global and public-private partnerships while reflecting the neoliberal trend of the decreasing role of the state, the increasing role of the private sector, privatization, and reliance on external funding.
5. Barriers of current interventions for HAT
Although global interventions for HAT have been a success, the goal of complete elimination by 2030 is ambitious. Major barriers include the adverse effect of success of recent global interventions, the difficulty in development of new medicine and vaccination, geographical and social factors, conflicts, and weak governance. As HAT approaches eradication after recent successful interventions, new challenges have emerged in the field, posing significant obstacles to ongoing interventions. Young medical professionals and laboratory personnel with less experience in HAT cases has led to a lack of appropriate awareness and knowledge about the disease. This results in usage of expired reagent, false negative test results, misdiagnoses, and delays in the start of treatment[lvii]. The decline in HAT cases has led to reduced public motivation to participate in mass screening campaigns, as well as decreased interest in eradication efforts among health system staff and funders. Additionally, changes in the socio-political environment made it harder to do the active mass screening for early detection by the PNLTHA mobile team who travels to endemic villages. During the Mobutu regime in 1965-1997, an era marked by significant HAT outbreaks, it was easier to get community members to come to the mobile team. Local leaders were also more inclined to help the mobile team since the authorities fined people who did not go[lviii]. Although the national HAT program in the DRC, the Programme National de Lutte contre la Trypanosomiase Humaine Africaine (PNLTHA), is heavily reliant on external funding[lix], the decreasing new cases of HAT can also severely impact international support and funding on HAT. Reorientation, disinvestment, and withdrawal from HAT projects by major donors have been raising concerns. Even the Belgian Development Agency (BTC-CTB), a key partner in combatting HAT, is planning on integrating HAT projects into existing health structures in the DRC. This is in line with the current international trend of integration of interventions on neglected tropical disease (NTD) into existing health structures. However, primary healthcare facilities in endemic areas where resources are scarce and conflict is prevalent, are lacking, let alone human resources and facilities for complicated surveillance and treatment[lx].
Another challenge is the difficulty, complexity, resource-intensive nature of screening, treatment, and development of new drugs and vaccines for HAT. Tong et al.[lxi] states that although active screening by mobile teams is more effective for early detection and they have enhanced accessibility to larger populations compared to passive screening at fixed health facilities, active screening is more complex and costly. Additionally, despite the innovative new medicines and diagnostic measures, HAT still requires specific and complex skills and equipment. The development of a HAT vaccine has been unsuccessful due to the parasite’s ability in the blood stream to frequently change its outer protein coat[lxii] and decreasing HAT patients. Unstable endemic areas including rural and conflict areas also makes clinical trials more challenging[lxiii].
While progress in medical tools is inevitably important, frontline staff working for PNLTHA in the DRC were more concerned about other challenges than technological limitations. They expressed concern over more fundamental and large-scale issues that enable them to put technology to use. First, there is the issue of limited work on vectors, insufficient coverage of the territory by PNLTHA’s active screening activities, and unmet conditions for using available tools. The second problem is lack of public awareness and poor community engagement, which makes it difficult to convince them to get tested. Local communities don’t always know how to identify the disease and there is mistrust in the health system and government authorities, which are connected to the underlying problem of weak governance in DRC. These factors led frontline workers to lack confidence in the elimination of HAT, contrasting with the view of international and national policy makers[lxiv].
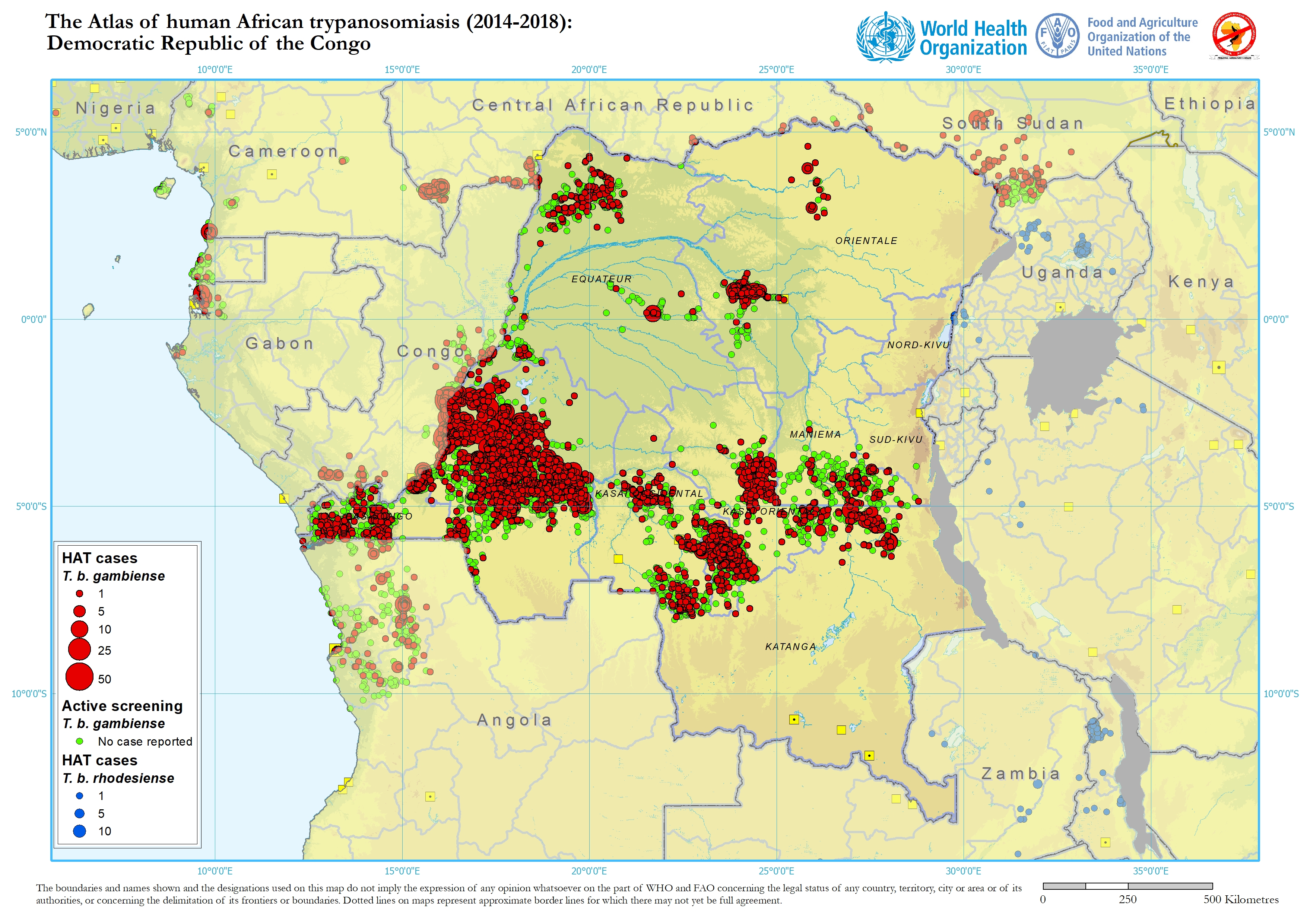
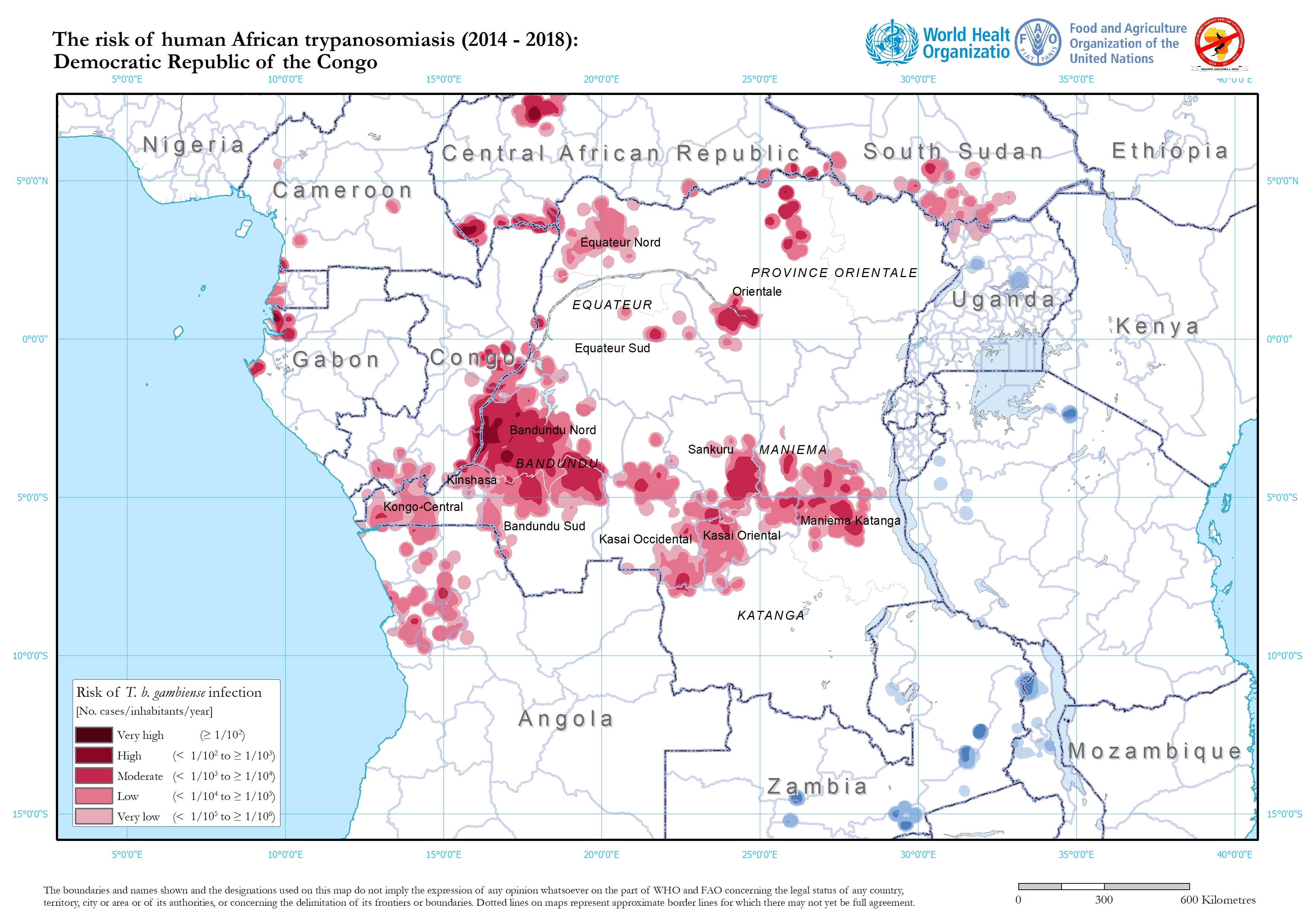
Weak governance in the DRC has allowed conflicts to persist, often overlapping with endemic areas where violence and political instability have severely disrupted HAT control, treatment, and follow-up efforts. This correlation is shown in Figure 7[lxv] and Figure 8[lxvi], particularly in the western region. Between 2007 and 2010, in the north-eastern region near the border, HAT screening and treatment projects were interrupted due to conflict. Additionally, migration of people due to evacuation from political instability and conflict raises the risk of spreading the disease, especially in border areas such as the north of the Orientale Province [lxvii] as seen in Figure 3[lxviii].
Considering these barriers, the limitations of current approaches is evident. While significant progress has been made in medical innovations and interventions, their success has been undermined by broader systemic and structural issues. These barriers underscore that addressing HAT is not solely a matter of advancing medical tools or strategies. Instead, it requires a holistic understanding of how social, political, and economic factors intersect with epidemiological challenges. Health-related analyses, including those on HAT, often overemphasize the medical and quantitative aspects, overlooking these critical underlying factors. However, as the persistence of HAT demonstrates, the goal of full elimination can only be achieved by addressing these deeper, structural barriers in tandem with medical efforts, both in analysis and implementation.
6. Conclusion
The historical trajectory of aid interventions for HAT in the DRC reveals the complex interplay between colonial policies, international collaboration, and the social and structural factors. Belgian colonial rule directly and indirectly influenced the spread of HAT. Initial interventions to control HAT were led by the colonial administration, which implemented strict measures that achieved some success. However, the post-independence turmoil led to a resurgence of HAT, which was later significantly reduced through drug development and large-scale aid interventions, serving as a notable example of international cooperation in public health. Despite these achievements, significant barriers remain, including challenges in drug development, ongoing conflicts, and a lack of trust in government authorities.
While the number of new cases has reached historic lows, medical innovations alone are insufficient to achieve the WHO’s ambitious goal of eliminating HAT by 2030. A holistic approach is essential, treating HAT not merely as a medical issue but as a broader social problem, addressing the systemic and structural barriers that hinder prevention, screening, and treatment efforts. Furthermore, complacency following successful control efforts risks a potential resurgence of the disease. Continued international and national attention, along with robust programs and sustained funding, remain crucial to preventing a relapse. The path toward HAT eradication transcends public health challenges; it requires continuous, comprehensive action to address the underlying social and structural determinants of the disease.
Figures
Figure 1:“Number of new reported cases of human African Trypanosomiasis”[i]

Figure 2:”Distribution of human African trypanosomiasis (T.b.gambiense), worldwide, 2023.” (WHO 2023)[ii]

Figure 3: Number of new reported cases of human African trypanosomiasis in DRC (T.b.gambiense):2023[iii]

Figure 4:Overview of new HAT cases from 1926-2018 (Mudji et, al, 2019)[iv]

Figure 5:Number of cases of African sleeping sickness reported (grey columns) and population screened (black circles)[v]

Figure 6:Conflict Watchlist 2024: Democratic Republic of the Congo[vi]

Figure 7:The Atlas of human African trypanosomiasis (2014-2018): Democratic Republish of the Congo[vii]

Figure 8:The risk of human African trypanosomiasis (2014-2018): Democratic Republic of the Congo[viii] (WHO 2024)

Achille Lutumba SuikaLiqiu, Anne Marie Nsaka KabundaZhang. 2016. “Evolution of African Human Trypanosomiasis in the Democratic Republic of Congo During the Year 2005.” American Journal of Environmental Protection. Vol. 5, No. 3, 2016, pp. 50-55.2016 doi: 10.11648/j.ajep.20160503.1. https://www.researchgate.net/profile/Achille-Lutumba-Suika/publication/346944504_Evolution_of_African_Human_Trypanosomiasis_in_the_Democratic_Republic_of_Congo_During_the_Year_2005/links/6086687c8ea909241e26305c/Evolution-of-African-Human-Trypanosomiasis-.
ACLED (Armed Conflict Location & Event Data). 2024. “Democratic Republic of Congo: Re-elected President Tshisekedi Faces Regional Crisis in the East.” https://acleddata.com/conflict-watchlist-2024/drc/.
Brun RJ, Chappuis F, Burri CBlum. 2010. “Human African trypanosomiasis.” “Lancet. 2010 Jan 9;375(9709):148-59. doi: 10.1016/S0140-6736(09)60829-1. Epub 2009 Oct 14. PMID: 19833383.”
Gao J-MZ-Y, Hide G, Lai D-H, Lun Z-R, Wu Z-DQian. 2020. “Human African trypanosomiasis: the current situation in endemic regions and the risks for non- endemic regions from imported cases.” Parasitology 147, 922–931. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7391876/pdf/S0031182020000645a.pdf.
HaskinM.Jeanne. 2005. “The Tragic State of the Congo from Decolonization to Dictatorship.” “Algora Publishing.” https://books.google.com/books?hl=ja&lr=lang_ja|lang_en&id=TKa2e3UvGMkC&oi=fnd&pg=PR3&dq=Democratic+Republic+of+the+Congo%E3%80%80colonization&ots=Ne_YfMzdR4&sig=hz4NL-G9GBYaif35k4wbz_pUNH4#v=onepage&q&f=false .
Hunt Rose Nancy. 1999. “Colonial Lexicon: Of Birth Ritual, Medicalization, and Mobility in the Congo.” Duke University Press.
International Atomic Energy Agency. 2002. “Campaign launched to Eliminate TseTse Fly.” https://www.iaea.org/newscenter/pressreleases/campaign-launched-eliminate-tsetse-fly.
Jacqueline Tong Valverde, Claude Mahoudeau, Oliver Yun and François ChappuisOlaf. 2011. “Challenges of controlling sleeping sickness in areas of violent conflict: experience in the Democratic Republic of Congo.” “Conflict and Health 5:7.” https://doi.org/10.1186/1752-1505-5-7.
Jean-Benoit Falisse Mwamba0Miaka, Alain MpanyaErick. 2020. “Whose Elimination? Frontline Workers’ Perspectives on the Elimination of the Human African Trypanosomiasis and Its Anticipated Consequences.” Trop. Med. Infect. Dis. 2020, 5,6; doi:10.3390/tropicalmed5010069.69-84. https://www.google.com/books/edition/Human_African_Trypanosomiasis_Sleeping_S/E9rrDwAAQBAJ?hl=ja&gbpv=1&dq=%22The+Atlas+of+Human+African+Trypanosomiasis&pg=PA42&printsec=frontcover.
Junior Mudji Benhamou, Erick Mwamba-Miaka, Christian Burri, Jojannes BlumJonathan. 2019. “The flipside of eradicating a Disease; Human African Trypanosomiasis in Woman in Rural Democratic Republic of Congo: A Case Report.” Trop. Med. Infect. Dis. 2019, 4, 142; doi:10.3390/tropicalmed40404021312. https://www.google.com/books/edition/Human_African_Trypanosomiasis_Sleeping_S/E9rrDwAAQBAJ?hl=ja&gbpv=1&dq=%22The+Atlas+of+Human+African+Trypanosomiasis&pg=PA42&printsec=frontcover.
Nzongola-Ntalaja Georges. 2002. “The Congo: From Leopold to Kabila: A People’s History.” Zed Books.
Philippe Neau Hanel, Valerie Lameyre, Nathalie Strub-Wourgaft and Luc KuykensHeinz. 2020. “Innovative Partnerships for the Elimination of Human African Trypanosomiasis and the Development of Fexinidazole.” Trop. Med. Infect. Dis.2020, 5,17; doi: 10.3390/tropicalmed5010817. 31-44. https://www.google.com/books/edition/Human_African_Trypanosomiasis_Sleeping_S/E9rrDwAAQBAJ?hl=ja&gbpv=1&dq=%22The+Atlas+of+Human+African+Trypanosomiasis&pg=PA42&printsec=frontcover.
R Daniel Headrick. 2014. “Sleeping sickness epidemics and colonial responses in East and Central Africa, 1900-1940.” “PLoS Negl Trop Dis. 2014 Apr 24;8(4):e2772. doi: 10.1371/journal.pntd.0002772. PMID: 24763309; PMCID: PMC3998934. 2014.” https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3998934/pdf/pntd.0002772.pdf.
Renton David Seddon, Leo Zeilig Dave,. 2007. “The Congo: Plunder and Resistance.” Zed Books.
Schroeder.Madeja and Ulrike Ulrich-Dietmar. 2020. “From Colonial Research Spirit to Global Commitment: Bayer and African Sleeping Sickness in the Mirror of History.” Trop. Med. Infect. Dis. 2020, 5,42, 161-167, 1st ed. New Yor Wiley. https://www.google.com/books/edition/Human_African_Trypanosomiasis_Sleeping_S/E9rrDwAAQBAJ?hl=ja&gbpv=1&dq=%22The+Atlas+of+Human+African+Trypanosomiasis&pg=PA42&printsec=frontcover.
Simarro PPA, Ruiz Postigo JA, Franco JR, Jannin JG.Diarra. 2011. “The human African trypanosomiasis control and surveillance programme of the World Health Organization 2000-2009: the way forward.” “PLoS Negl Trop Dis. 2011 Feb 22;5(2):e1007. doi: 10.1371/journal.pntd.0001007. PMID: 21364972; PMCID: PMC3042999.” https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3042999/pdf/pntd.0001007.pdf.
Steverding D. 2008. “The history of African trypanosomiasis.” “Parasites Vectors 1, 3.” https://doi.org/10.1186/1756-3305-1-3.
Tong Valverde, O., Mahoudeau, C., Yun, O., Chappuius, FJ.,. 2011. “Challenges of controlling sleeping sickness in areas of violent conflict: experience in the Democratic Republic of Congo.” “Confl Health 5, 7.” https://conflictandhealth.biomedcentral.com/articles/10.1186/1752-1505-5-7.
U.S. Committee for Refugees and Immigrants. 2020. “The Crisis in the Democratic Republic of the Congo.” https://refugees.org/wp-content/uploads/2020/12/USCRI-Backgrounder_DRC.pdf.
Vansina Jan. 2010. “Being Colonized: The Kuba Experience in Rural Congo, 1880–1960.” “Univ of Wisconsin Press.” https://books.google.com/books?hl=ja&lr=lang_ja|lang_en&id=mYRwo8SqqRwC&oi=fnd&pg=PR5&dq=Democratic+Republic+of+the+Congo+health+colonisation&ots=_as4-KiAfS&sig=xJNwdcg9Q9EBD5x2AIguzHfTMp0#v=onepage&q&f=false.
World Health Assembly. 1983. “Thirty-sixth World Health Assembly- African Human Trypanosomiasis.” https://iris.who.int/bitstream/handle/10665/160638/WHA36_R31_eng.pdf.
World Health Organization. 2023. “Human African trypanosomiasis, Number of new reported cases of human African trypanosomiasis (T.b.gambiense):2023.” https://apps.who.int/neglected_diseases/ntddata/hat/hat.html.
World Health Organization. 2024. “The Atlas of human African trypanosomiasis (2014-2018): Democratic Republic of the Congo.” http://quarry.essi.upc.edu:8080/who/Distribution/HAT_DRC_2014-2018.jpg.
{kind=link}
World Health Organization. 2024. “The risk of human African trypanosomiasis (2014-2018): Democratic Republic of the Congo.” http://quarry.essi.upc.edu:8080/who/Risk/Risk_DRC_2014-2018.jpg.
{kind=link}
[i] World Health Organization. 2023. “Human African trypanosomiasis, Number of new reported cases of human African trypanosomiasis (T.b.gambiense):2023.” https://apps.who.int/neglected_diseases/ntddata/hat/hat.html.
[ii] Ibid.
[iii] Philippe Neau Hanel, Valerie Lameyre, Nathalie Strub-Wourgaft and Luc KuykensHeinz. 2020. “Innovative Partnerships for the Elimination of Human African Trypanosomiasis and the Development of Fexinidazole.” Trop. Med. Infect. Dis.2020, 5,17; doi: 10.3390/tropicalmed5010817. 31-44. https://www.google.com/books/edition/Human_African_Trypanosomiasis_Sleeping_S/E9rrDwAAQBAJ?hl=ja&gbpv=1&dq=%22The+Atlas+of+Human+African+Trypanosomiasis&pg=PA42&printsec=frontcover.
[iv] Ibid.
[v] R Daniel Headrick. 2014. “Sleeping sickness epidemics and colonial responses in East and Central Africa, 1900-1940.” “PLoS Negl Trop Dis. 2014 Apr 24;8(4):e2772. doi: 10.1371/journal.pntd.0002772. PMID: 24763309; PMCID: PMC3998934. 2014.” https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3998934/pdf/pntd.0002772.pdf.
[vi] Vansina Jan. 2010. “Being Colonized: The Kuba Experience in Rural Congo, 1880–1960.” “Univ of Wisconsin Press.” https://books.google.com/books?hl=ja&lr=lang_ja|lang_en&id=mYRwo8SqqRwC&oi=fnd&pg=PR5&dq=Democratic+Republic+of+the+Congo+health+colonisation&ots=_as4-KiAfS&sig=xJNwdcg9Q9EBD5x2AIguzHfTMp0#v=onepage&q&f=false.
[vii] U.S. Committee for Refugees and Immigrants. 2020. “The Crisis in the Democratic Republic of the Congo.” https://refugees.org/wp-content/uploads/2020/12/USCRI-Backgrounder_DRC.pdf.
[viii] HaskinM.Jeanne. 2005. “The Tragic State of the Congo from Decolonization to Dictatorship.” Algora Publishing. https://books.google.com/books?hl=ja&lr=lang_ja|lang_en&id=TKa2e3UvGMkC&oi=fnd&pg=PR3&dq=Democratic+Republic+of+the+Congo%E3%80%80colonization&ots=Ne_YfMzdR4&sig=hz4NL-G9GBYaif35k4wbz_pUNH4#v=onepage&q&f=false
[ix] Steverding D. 2008. “The history of African trypanosomiasis.” Parasites Vectors 1, 3. https://doi.org/10.1186/1756-3305-1-3.
[x] Ibid.
[xi] Brun RJ, Chappuis F, Burri CBlum. 2010. “Human African trypanosomiasis.”Lancet. 2010 Jan 9;375(9709):148-59. doi: 10.1016/S0140-6736(09)60829-1. Epub 2009 Oct 14. PMID: 19833383.
[xii] Nzongola-Ntalaja Georges. 2002. “The Congo: From Leopold to Kabila: A People’s History.” Zed Books.
[xiii] U.S. Committee for Refugees and Immigrants. 2020.
[xiv] Renton David Seddon, Leo Zeilig Dave,. 2007. “The Congo: Plunder and Resistance.” Zed Books.
[xv] Hunt Rose Nancy. 1999. “Colonial Lexicon: Of Birth Ritual, Medicalization, and Mobility in the Congo.” Duke University Press.
[xvi] World Health Organization. 2023.
[xvii] Vansina Jan. 2010.
[xviii] Steverding D. 2008.
[xix] Renton David Seddon, Leo Zeilig Dave,. 2007.
[xx] U.S. Committee for Refugees and Immigrants. 2020.
[xxi] Jacqueline Tong Valverde, Claude Mahoudeau, Oliver Yun and François ChappuisOlaf. 2011. “Challenges of controlling sleeping sickness in areas of violent conflict: experience in the Democratic Republic of Congo.” “Conflict and Health 5:7.” https://doi.org/10.1186/1752-1505-5-7.
[xxii] Steverding D. 2008.
[xxiii] Achille Lutumba SuikaLiqiu, Anne Marie Nsaka KabundaZhang. 2016. “Evolution of African Human Trypanosomiasis in the Democratic Republic of Congo During the Year 2005.” American Journal of Environmental Protection. Vol. 5, No. 3, 2016, pp. 50-55.2016 doi: 10.11648/j.ajep.20160503.1. https://www.researchgate.net/profile/Achille-Lutumba-Suika/publication/346944504_Evolution_of_African_Human_Trypanosomiasis_in_the_Democratic_Republic_of_Congo_During_the_Year_2005/links/6086687c8ea909241e26305c/Evolution-of-African-Human-Trypanosomiasis-.
[xxiv] R Daniel Headrick. 2014.
[xxv] Simarro PPA, Ruiz Postigo JA, Franco JR, Jannin JG.Diarra. 2011. “The human African trypanosomiasis control and surveillance programme of the World Health Organization 2000-2009: the way forward.” PLoS Negl Trop Dis. 2011 Feb 22;5(2):e1007. doi: 10.1371/journal.pntd.0001007. PMID: 21364972; PMCID: PMC3042999. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3042999/pdf/pntd.0001007.pdf.
[xxvi] Ibid.
[xxvii] Steverding D. 2008.
[xxviii] Ibid.
[xxix] R Daniel Headrick. 2014.
[xxx] Ibid.
[xxxi] Steverding D. 2008.
[xxxii] Ibid.
[xxxiii] Ibid.
[xxxiv] Jean-Benoit Falisse Mwamba0Miaka, Alain MpanyaErick. 2020. “Whose Elimination? Frontline Workers’ Perspectives on the Elimination of the Human African Trypanosomiasis and Its Anticipated Consequences.” Trop. Med. Infect. Dis. 2020, 5,6; doi:10.3390/tropicalmed5010069.69-84. https://www.google.com/books/edition/Human_African_Trypanosomiasis_Sleeping_S/E9rrDwAAQBAJ?hl=ja&gbpv=1&dq=%22The+Atlas+of+Human+African+Trypanosomiasis&pg=PA42&printsec=frontcover.
[xxxv] Steverding D. 2008.
[xxxvi] R Daniel Headrick. 2014.
[xxxvii] Jean-Benoit Falisse Mwamba0Miaka, Alain MpanyaErick. 2020.
[xxxviii] Steverding D. 2008.
[xxxix] Gao J-MZ-Y, Hide G, Lai D-H, Lun Z-R, Wu Z-DQian. 2020. “Human African trypanosomiasis: the current situation in endemic regions and the risks for non- endemic regions from imported cases.” Parasitology 147, 922–931. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7391876/pdf/S0031182020000645a.pdf.
[xl] Steverding D. 2008.
[xli] Simarro PPA, Ruiz Postigo JA, Franco JR, Jannin JG.Diarra. 2011.
[xlii] Schroeder.Madeja and Ulrike Ulrich-Dietmar. 2020. “From Colonial Research Spirit to Global Commitment: Bayer and African Sleeping Sickness in the Mirror of History.” “Trop. Med. Infect. Dis. 2020, 5,42, 161-167, 1st ed. New Yor Wiley.” https://www.google.com/books/edition/Human_African_Trypanosomiasis_Sleeping_S/E9rrDwAAQBAJ?hl=ja&gbpv=1&dq=%22The+Atlas+of+Human+African+Trypanosomiasis&pg=PA42&printsec=frontcover.
[xliii] Ibid.
[xliv] Simarro PPA, Ruiz Postigo JA, Franco JR, Jannin JG.Diarra. 2011.
[xlv] Schroeder.Madeja and Ulrike Ulrich-Dietmar. 2020.
[xlvi] World Health Assembly. 1983. “Thirty-sixth World Health Assembly- African Human Trypanosomiasis.” https://iris.who.int/bitstream/handle/10665/160638/WHA36_R31_eng.pdf.
[xlvii] Gao J-MZ-Y, Hide G, Lai D-H, Lun Z-R, Wu Z-DQian. 2020.
[xlviii] Philippe Neau Hanel, Valerie Lameyre, Nathalie Strub-Wourgaft and Luc KuykensHeinz. 2020.
[xlix] Ibid.
[l] Simarro PPA, Ruiz Postigo JA, Franco JR, Jannin JG.Diarra. 2011.
[li] Schroeder.Madeja and Ulrike Ulrich-Dietmar. 2020.
[lii] Simarro PPA, Ruiz Postigo JA, Franco JR, Jannin JG.Diarra. 2011.
[liii] World Health Organization. 2023.
[liv] Ibid.
[lv] Philippe Neau Hanel, Valerie Lameyre, Nathalie Strub-Wourgaft and Luc KuykensHeinz. 2020.
[lvi] Ibid.
[lvii] Junior Mudji Benhamou, Erick Mwamba-Miaka, Christian Burri, Jojannes BlumJonathan. 2019. “The flipside of eradicating a Disease; Human African Trypanosomiasis in Woman in Rural Democratic Republic of Congo: A Case Report.” Trop. Med. Infect. Dis. 2019, 4, 142; doi:10.3390/tropicalmed40404021312. https://www.google.com/books/edition/Human_African_Trypanosomiasis_Sleeping_S/E9rrDwAAQBAJ?hl=ja&gbpv=1&dq=%22The+Atlas+of+Human+African+Trypanosomiasis&pg=PA42&printsec=frontcover.
[lviii] Jean-Benoit Falisse Mwamba0Miaka, Alain MpanyaErick. 2020.
[lix] Ibid.
[lx] Jacqueline Tong Valverde, Claude Mahoudeau, Oliver Yun and François ChappuisOlaf. 2011.
[lxi] Ibid.
[lxii] International Atomic Energy Agency. 2002. “Campaign launched to Eliminate TseTse Fly.” https://www.iaea.org/newscenter/pressreleases/campaign-launched-eliminate-tsetse-fly.
[lxiii] Jacqueline Tong Valverde, Claude Mahoudeau, Oliver Yun and François ChappuisOlaf. 2011.
[lxiv] Jean-Benoit Falisse Mwamba0Miaka, Alain MpanyaErick. 2020.
[lxv] ACLED (Armed Conflict Location & Event Data). 2024. “Democratic Republic of Congo: Re-elected President Tshisekedi Faces Regional Crisis in the East.” https://acleddata.com/conflict-watchlist-2024/drc/.
[lxvi] World Health Organization. 2024. “The risk of human African trypanosomiasis (2014-2018): Democratic Republic of the Congo.” http://quarry.essi.upc.edu:8080/who/Risk/Risk_DRC_2014-2018.jpg.
[lxvii] Jacqueline Tong Valverde, Claude Mahoudeau, Oliver Yun and François ChappuisOlaf. 2011.
[lxviii] World Health Organization. 2023.
[lxix] Ibid.
[lxx] Ibid.
[lxxi] Ibid.
[lxxii] Junior Mudji Benhamou, Erick Mwamba-Miaka, Christian Burri, Jojannes BlumJonathan. 2019.
[lxxiii] Schroeder.Madeja and Ulrike Ulrich-Dietmar. 2020.
[lxxiv] ACLED (Armed Conflict Location & Event Data). 2024.
[lxxv] World Health Organization. 2024. “The Atlas of human African trypanosomiasis (2014-2018): Democratic Republic of the Congo.” http://quarry.essi.upc.edu:8080/who/Distribution/HAT_DRC_2014-2018.jpg.
[lxxvi] World Health Organization. 2024.
ABOUT AUTHOR/S

Natsuko Matsukawa
Natsuko Matsukawa is a first-year graduate student from Japan in the International Development Program at SIS. Her concentration is in Global Health, particularly NCDs (Non-communicable diseases).
Leave a Reply